|
Flashes of light or spots in one's vision (floaters), are generally innocuous, having typical causes and causing no harm in and of themselves. However, the sudden onset of flashers or an increase in floaters, particularly accompanied by flashes of light, can be an indication of more serious eye problems such as a retinal tear or detachment. If you experience these symptoms, please schedule an appointment that day, if possible.
The three basic types of retinal detachment are rhegmatogenous, tractional and exudative.
Rhegmatogenous Retinal Detachment
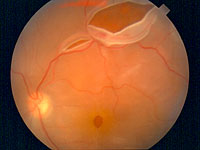
Rhegmatogenous retinal detachment is the most common form of detachment. In this condition, a tear, hole or break in the retina enables fluid to enter the subretinal space between the sensory retina and the retinal pigment epithelium (RPE) beneath the retina, causing the retina to separate from the layer beneath it. The retina receives oxygen and nutrients from this tissue and will begin to lose function and ultimately die if it remains detached. Retinal detachment of this type is an emergency with surgery usually scheduled on an urgent basis within 24 hours of the diagnosis.
Most cases of this type of retinal detachment are associated with the natural aging process. The separation that occurs can occasionally be accelerated by cataract surgery, YAG laser capsulotomy following cataract surgery, diabetes, trauma, hemorrhage within the eye and uveitis (inflammation within the eye). Certain conditions including a number of inherited syndromes, a peripheral retinal degeneration (lattice degeneration), or extreme nearsightedness (myopia) may predispose individuals to retinal detachment.
Symptoms
Symptoms of the onset of this condition include flashes of light, floaters and a curtain-like loss of vision as detachment develops. It is extremely important to seek immediate treatment if these symptoms develop. The patient's visual acuity prior to treament correlates with postoperative visual acuity; in other words, the sooner treatment is sought and the more vision that is retained prior to surgery, the more vision will be retained or restored following surgery. In more than 90% of cases, retinal detachment surgery is successful in reattaching the retina.
Treatment
The three surgical methods most used to treat rhegmatogenous retnial detachment are: the placement of an encircling band around the eye (scleral buckling); surgical removal of the vitreous humor (vitrectomy) in which the natural gel-like fluid filling the center cavity of the eye is removed and then replaced to maintain correct pressure; and, the injection of a gas bubble into the vitreous cavity (pneumatic retinopexy) along with cryotherapy (the therapeutic use of cold temperature treatment) of the retinal break.
 Back to Top Back to Top
Tractional Retinal Detachment
This type of retinal detachment takes place when fibrous membrane in the vitreous humor and retina causes traction on the retina, pulling the retina from the layer beneath (the retinal pigment epithelium or RPE). This type of detachment is most common in proliferative diabetic retinopathy, the advanced stages of diabetic retinopathy.
Symptoms
Its symptoms are usually blind spots and/or loss of vision. Flashes of light, floaters and a curtain-like vision loss are experienced by some patients.
Treatment
Treatment necessitates relieving the traction which is causing the detachment and usually requires removal of the vitreous humor and tractional membranes. The intraocular injection of air, gas or silicone oil may help prevent recurrent retinal detachment in some patients. Prognosis may be guarded in patients with severe underlying retinopathy.
Back to Top
Exudative Retinal Detachment
Exudative retinal detachment is associated with conditions that affect the blood- retinal barrier, allowing the build-up of fluid beneath the retina without the presence of a hole, tear or break. Inflammatory conditions may contribute to the development of the condition along with tumors of the eye and congenital abnormalities.
Treatment
Treatment of this type of retinal detachment is often non-surgical because it is frequently the underlying systemic condition that requires treatment. If timely treatment is able to be rapidly control the underlying condition, the patient's prognosis for recovery of vision can be good.
Testing
Diagnostic testing for retinal detachment may include: a pupil reflex test, visual acuity test, slit-lamp examination, ophthalmoscopy, and ultrasound examination. If retinal detachment is suspected, the doctor will administer all appropriate testing to determine its cause and proper treatment.
Back to Top
|