|
Individuals with diabetes do expereince a higher risk of blindness than those without the disease. But the majority of people with diabetes have only minor eye disorders. With regular eye exams and early diagnosis, even if a major problem develops, there are treatments that can work well.
Following are certain eye conditions to which those with diabetes are more susceptible:
Glaucoma
Glaucoma is 40% more likely to occur in people with diabetes than those without. Glaucoma is increasingly common the longer a person has had diabetes. Risk increases with age, as well.
Glaucoma occurs due to a buildup of pressure in the eye. Pressure is caused by the buildup of aqueous humor (fluid) in the anterior chamber of the eye. In turn, the pressure compresses the blood vessels that take blood flow to the retina and optic nerve, which is necessary for vision. The retina and optic nerve become damaged and vision is gradually lost.
Glaucoma can be treated in a number of ways. Depending on the severity of the case, drugs may be used to reduce internal eye pressure or surgery may be needed.
You may read further about this eye disease and the treatment we offer by going to the link on glaucoma on our home page.
 Back to Top Back to Top
Cataracts
When cataracts develop, light is blocked because the clear lens of the eye becomes cloudy. People with diabetes are 60% more likely to develop cataracts than those who do not have diabetes. They also have a tendency to develop cataracts at a younger age, with faster progression.
With cataracts that are mild, the condition is usually monitored. If cataracts interfere with vision, surgery may be recommended to remove and replace the lens of the eye. In those with diabetes, there is the risk that retinopathy can worsen after removal of the lens and that glaucoma may begin to develop.
You may read more about our treatment for cataracts by clicking on the link for that section on our home page.
Back to Top
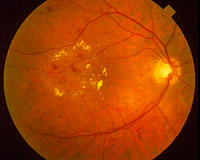
Retinopathy
All disorders of the retina caused by diabetes come under the general term, diabetic retinopathy. The two main types of retinopathy are nonproliferative and proliferative.
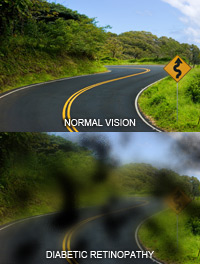
Nonproliferative retinopathy is the most common form. In this condition, small blood vessels in the back of the eye swell and form pouches. Nonproliferative retinopathy moves through three stages as blockage occurs in more and more blood vessels. While vision loss does not usually occur at this stage, capillary walls can lose their ability to regulate the passage of substances between the blood and the retina. Fluid can then leak into the macula, the part of the eye where focusing takes place. Once the macula swells with fluid, the vision blurs in a condition called macula edema. Nonproliferative retinopathy generally requires treatment but macular edema must be treated. Treatment has proven effective in stopping and, at times, reversing loss of vision.
Proliferative retinopathy is a more serious form of retinopathy to which some patients may progress after several years. The blood vessels become so damaged that they close off. In reaction, new blood vessels begin growing in the retina but they are weak. They can leak blood which blocks the vision in a condition known as vitreous hemorrhage. Additionally, these new blood vessels can cause the growth of scar tissue. Once scar tissue shrinks, it can cause retinal detachment, distorting the retina or pulling it out of place.
It is possible for your retina to suffer extensive damage prior to noting any change in vision. The majority of those with nonproliferative retinopathy do not have symptoms. And even with the more debilitating proliferative retinopathy, there may be no symptoms. This is why it is so important to have regular exams by an ophthalmologist.
The length of time you have had diabetes, your blood sugar levels, blood sugar control, blood pressure control, and your genes all influence your likelihood of getting retinopathy.
You are more likely to have retinopathy the longer you've had diabetes. Nearly all of those with type 1 diabetes will ultimately have nonproliferative retinopathy. Most people with type 2 diabetes will also get it. The incidence of the more destructive proliferative retinopathy is much more infrequent.
Maintaining your blood sugar levels closer to normal will make you less disposed to have retinopathy or more likely to get a milder form.
Back to Top
Treatment
The treatment of diabetic retinopathy has greatly advanced. Treatment enjoys the greatest success with early diagnosis. In most patients, procedures like scatter photocoagulation, focal photocoagulation, and vitrectomy are able to prevent blindness. It is while the patient's sight is still normal that the best results are obtained.
Photocoagulation — A special laser is used to create tiny burns under the retina. The burns seal the blood vessels to stop them from growing and leaking.
Scatter Photocoagulation — Also known as panretinal photocoagulation. The doctor uses the laser to create a polka-dot pattern of hundreds of tiny burns in two or more treatments. If scatter photocoagulation is used prior to bleeding or retinal detachment having progressed too far, it reduces the risk of blindness from vitreous hemorrhage or detachment. Neovascular glaucoma is treated using the same procedure.
Side effects of this procedure are generally minor. They can include a number of days of blurred vision following each treatment and the possible loss of peripheral (side) vision.
Focal Photocoagulation — In this procedure, the doctor precisely aims the laser at leaking blood vessels in the macula (a small, extremely important area in the back of the eye which provides sharp, central vision to see in fine detail, to read, and to drive). Treatment may prevent blurry vision caused by macular edema from getting worse.
Vitrectomy — This surgery removes cloudy fluid and scar tissue from within the eye. It is an option used when a lot of blood has leaked into the eye or the retina has already detached, rendering photocoagulation no longer effective. The operation enjoys better results the earlier it is performed. Reattaching the retina is a difficult procedure and the surgery is about 50% effective when used for that purpose. When used for removal of blood from the eye, it has a high rate of success.
Injection Therapy — Injectable medication therapy is used to reduce the amount of swelling in the macula; a consequence of uncontrolled diabetes. The two drug classes that have shown promise in reducing diabetic macular edema and retinopathy are Steroids and Anti vascular endothelial growth factor (Anti-VEGF). The goal of these drugs are to reduce inflammation and the growth of abnormal leaky blood vessels from forming, thus helping slow vision loss.
New forms of treatment are currently under clinical trials and the future seems bright.
Back to Top
|